
Abstract
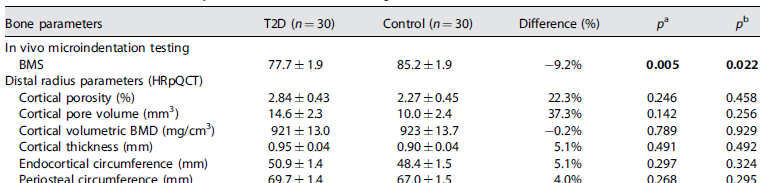
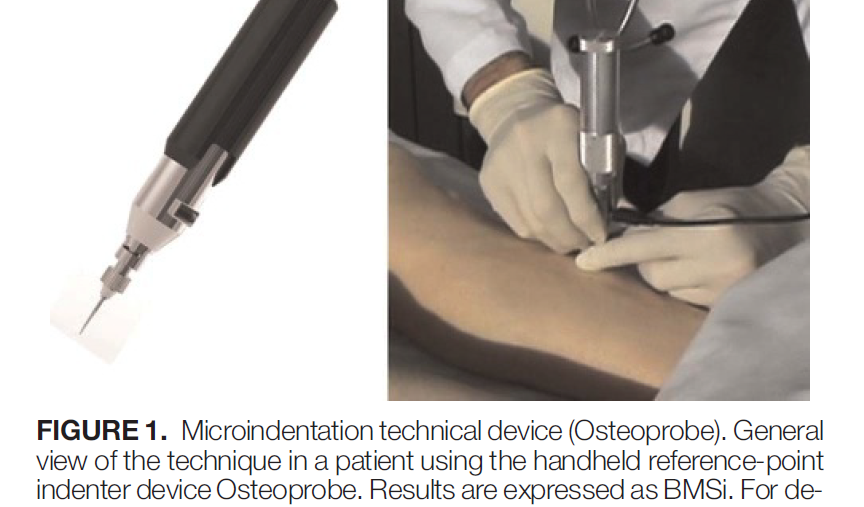
Although patients with type 2 diabetes (T2D) are at significant risk for well-recognized diabetic complications, including macrovascular disease, retinopathy, nephropathy, and neuropathy, it is also clear that T2D patients are at increased risk for fragility fractures. Furthermore, fragility fractures in patients with T2D occur at higher bone mineral density (BMD) values compared to nondiabetic controls, suggesting abnormalities in bone material strength (BMS) and/or bone microarchitecture (bone “quality”). Thus, we performed in vivo microindentation testing of the tibia to directly measure BMS in 60 postmenopausal women (age range, 50-80 years) including 30 patients diagnosed with T2D for >10 years and 30 age-matched, nondiabetic controls. Regional BMD was measured by dual-energy X-ray absorptiometry (DXA); cortical and trabecular bone microarchitecture was assessed from high-resolution peripheral quantitative computed tomography (HRpQCT) images of the distal radius and tibia. Compared to controls, T2D patients had significantly lower BMS: unadjusted (-11.7%; p<0.001); following adjustment for body mass index (BMI) (-10.5%; p<0.001); and following additional adjustment for age, hypertension, nephropathy, neuropathy, retinopathy, and vascular disease (-9.2%; p=0.022). By contrast, after adjustment for confounding by BMI, T2D patients had bone microarchitecture and BMD that were not significantly different than controls; however, radial cortical porosity tended to be higher in the T2D patients. In addition, patients with T2D had significantly reduced serum markers of bone turnover (all p<0.001) compared to controls. Of note, in patients with T2D, the average glycated hemoglobin level over the previous 10 years was negatively correlated with BMS (r=-0.41; p=0.026). In conclusion, these findings represent the first demonstration of compromised BMS in patients with T2D. Furthermore, our results confirm previous studies demonstrating low bone turnover in patients with T2D and highlight the potential detrimental effects of prolonged hyperglycemia on bone quality. Thus, the skeleton needs to be recognized as another important target tissue subject to diabetic complications.
https://www.ncbi.nlm.nih.gov/pubmed/24123088
J Bone Miner Res. 2014 Apr;29(4):787-95. doi: 10.1002/jbmr.2106.

{kind=link}